A man has been reunited with staff from London Ambulance Service who saved his life after he collapsed at home in cardiac arrest.
Andreas Kallis, 68, and his family visited Walthamstow ambulance station recently for the opportunity to meet and personally thank all those involved.
His wife Tina, 63, recalls the moment her daughter, Christina, 37, alerted her to Andreas’s collapse at their home back in February 2018: “All of a sudden my daughter came to me and said: ‘Mum, I don’t know if dads asleep or ignoring me’.”
After running into the sitting room and checking if he was breathing, they immediately dialled 999. They spoke to Emergency Call Coordinator, Fran De Wet, working in the London Ambulance Service control room, who started directing them through cardiopulmonary resuscitation (CPR).
“Fran told us precisely how to do CPR and the rhythm as well. I did so much better than I thought and that’s because of her help.”
An ambulance was quickly dispatched and London Ambulance Service paramedic crew Esme Choonara and Amanda Gowing responded to the scene.
They managed to get a pulse and rushed Andreas into Barts Heart Centre at St Bartholomew’s Hospital, where with the help of doctors and nurses has made a full recovery.
At the emotional reunion Andreas and Tina were joined by Fran, Esme and Amanda.
Andreas said: “I must be really lucky to survive. If it wasn’t for the London Ambulance Service, my wife and daughter I wouldn’t be here now. It was wonderful to be able to thank them all personally.”
Call handler Fran said: “This is why we do the job. That feeling of knowing that something you’ve done has really helped someone and their family.”
“In over twelve years working for the Service I have taken several cardiac arrest calls. But I have only ever received three letters to tell me that those patients have returned to normal life and have walked out of hospital. So to actually meet Mr Kallis is truly amazing.
“The whole experience has been overwhelming – I promised I wouldn’t cry but I did.”
The family wants to raise awareness of the importance of the general public learning lifesaving skills such as CPR. Tina said: “I had done a bit of CPR training years ago, but you never really think that something like this is going to happen to you.
“I just feel so good that I was able to help save him.”
“We are so grateful to all of the ambulance staff and everyone at St Bartholomew’s Hospital, the nurses, the doctors and the police who also attended that day. It feels like it is the closure we needed. To thank them and to see them in lovely surroundings not in that traumatic, horrendous way.”
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-09 10:55:582019-08-13 11:18:00"If it wasn't for the London Ambulance Service, my wife and daughter, I wouldn't be here now." Chingford cardiac arrest survivor thanks staff who saved his life
Improving the chances of survival for cardiac arrest patients is something close to North East Ambulance Service’s heart and their latest initiative is set to do just that.
If you or someone you cared about was having a cardiac arrest and just a short walk away from where you were, there was someone trained in lifesaving skills, would you want them to come and help?
Approximately 60,000 people suffer a cardiac arrest out of hospital in England every year and of these, 28,000 patients will have resuscitation started or continued by the ambulance service. Survival rates for these patients is 8.6%. This is significantly lower than for populations in other developed countries like Holland (21%), Seattle (20%) and Norway (25%).
The current rate of initial bystander CPR in England is reported as being 43% compared to up to 73% in other countries.
North East Ambulance Service has now switched on GoodSam, a mobile app that alerts community first responders to an incident, in an attempt to boost the numbers of people who survive cardiac arrest in the region.
GoodSAM connects with a community of first aid trained responders, willing to assist during a cardiac arrest.
NEAS will be switching on the system in the North East and inviting its clinically trained staff, trained in basic first aid and qualified to perform lifesaving cardiopulmonary resuscitation, to register initially.
GoodSAM will automatically notify nearby GoodSAM responders of a medical emergency. The platform connects those in need with those who have the skills to provide critical help before the emergency services arrive. The app is free to download on all smartphones.
GoodSAM is already working in partnership with ambulance services in London, North West, Wales and East Midlands as well as further afield in Australia, New Zealand, Ireland, USA, Canada and South Africa.
Gareth Campbell, Clinical Operations Manager says, “This is excellent news for the North East population and means that those special skills our workforce uses every day to help save lives are even more accessible. By ensuring a patient has a clear airway and quality CPR is in place in those first few minutes, they are more likely to achieve a good outcome.”
With the system now switched on, the NEAS emergency operations centre will alert the three nearest responders to life threatening incidents and simultaneously dispatch an ambulance, giving the patient the best possible chance of survival. The partnership will not impact on or substitute standard ambulance dispatch, with crews continuing to be sent to scene in the usual way.
When a volunteer is alerted, they will be able to accept the alert via the GoodSAM app and make their way to the location of the incident. If a volunteer responder is not in a position to accept the alert, it can be declined and diverted to the next nearest responder.
Campbell continues, “Having seen how successfully this app works elsewhere, we wanted to bring GoodSAM to the North East for the benefit of our region’s patients. Thanks to funding from NESTA, we have been able to work in partnership with the GoodSAM team to bring this app to the North East.”
NEAS already has a team of Community First Responders who are everyday members of the general public trained by NEAS in basic first aid and life support. They are provided with oxygen and a defibrillator and are deployed by NEAS to life threatening emergencies, such as chest pain, breathing difficulties, cardiac arrests, and unconsciousness, if they are the nearest resource, followed by the next nearest emergency care crew.
This app provides an opportunity for those with first aid skills who volunteer and work for the service to join the robust community of first responders already working within the North East.
Campbell adds, “Responders will be able to provide immediate care to a patient where every second counts, administering life-saving first aid while an ambulance is on its way. A patient who suffers a cardiac arrest stands a much better chance of survival if someone with a defibrillator can attend the patient in the first minutes of collapse.”
Professor Mark Wilson, GoodSAM’s Medical Director and Co-Founder, said: “If a patient has a cardiac arrest, it’s the first few minutes after the incident that determine the outcome – life, death, or long-term brain damage”.
“There are first aid trained people all around us but usually the first they know of a neighbour having a cardiac arrest is an ambulance appearing in their street. Our work with Ambulance Services, allows us to harness the lifesaving skills in the minutes before ambulance arrival. GoodSAM has saved lives globally and we look forward to working with NEAS to bring the benefits to the North East.”
Steve Dunn from Newton Aycliffe in County Durham has been a community first responder in the North East for eight years after he found himself coincidentally at the scene of two serious road traffic collisions in which he assisted patients whilst an ambulance was travelling. Having formerly been registered with GoodSam in London, he’s really pleased to be able to connect in his own region.
He explains, “I was alerted by GoodSAM to an incident in St Pancras when I was in London recently on a business trip and I was really overwhelmed by the number of people nearby who also got the alert. I was first on scene and between those of us who attended, the patient had the best chance of a good outcome. On this occasion it wasn’t a cardiac arrest luckily. It was really surprising and reassuring that so many people were willing to stop what they were doing and help and it’s great that we can do the same here.”
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-08 15:26:502019-08-13 11:18:30Improving the chances of surviving a cardiac arrest in the North East
Published in: Summer 2019 Edition of Ambulance Today Magazine
“When you’re compassionate, you’re not running away from suffering, you’re not feeling overwhelmed by suffering, and you’re not pretending the suffering doesn’t exist. When you are practicing compassion, you can stay present with suffering.”
Sara Shairer: https://eftraining.co.uk/what-is-compassion-fatigue/
In the emergency first responder profession, where we witness trauma first-hand, it is at times difficult to be fully aware of the impact that “direct trauma” has on us as practitioners and how to differentiate between direct trauma and vicarious trauma. Research suggests that EMS personnel experience many reactions after exposure to a traumatic event. Admitting to being emotionally affected is regarded as difficult as it may lead to being perceived by their peers as not tough enough for the job. The attitude of ‘no one dies on my watch’ is common amongst EMS personnel. This leads to EMS personnel often suppressing their emotions and feelings associated with the reality of their work in order to live up to this image of being strong and resilient.
“Injury mortality rates in South Africa are approximately six times higher than the global average. One of a handful of studies conducted amongst EMS personnel in the Western Cape found higher prevalence of exposure to critical incidents compared to their counterparts in other low-income countries.”
African Journal of Emergency Medicine Volume 5, Issue 1, March 2015
This Quarter we attempt to unpack and understand the lived experiences of compassion fatigue, vicarious/secondary trauma (ST), and burnout.
These three terms are complementary and yet different from one another.
-Compassion Fatigue (CF): Also called “vicarious traumatization” or secondary traumatization (Figley, 1995). The emotional residue or strain of exposure to working with those suffering from the consequences of traumatic events. It differs from burn-out but can co-exist. Compassion Fatigue can occur due to exposure on one case or can be due to a “cumulative” level of trauma.
The American Institute of Stress - https://www.stress.org
-Vicarious Trauma (VT): is a process of change resulting from empathetic engagement with trauma survivors. Anyone who engages empathetically with survivors of traumatic incidents, torture, and material relating to their trauma, is potentially affected.
-Burnout: a “syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed. It is characterized by three dimensions: 1) feelings of energy depletion or exhaustion; 2) increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job; and 3) reduced professional efficacy.
The American Institute of Stress - https://www.stress.org
Despite the differing theories and terminology of the three concepts, each is directly associated with the concept of empathy. There are two key components:cognitive empathy, the ability to take someone’s perspective, and affective empathy, whereby an individual share a similar emotional response to others’ experiences(Smith, 2006).
With empathy holding sway as a common factor in CF, VT and burnout, it would make sense then to conclude that cognitive and affective empathy would impact differently on the life of the practitioner. For example, a professional empathising emotionally may experience more emotional consequences than an individual empathising cognitively. In addition to increased experiences of trauma, increased case load and less clinical experience, it is therefore suggested that the nature of empathetic engagement in work-related scenarios would therefore be an important dimension to consider in understanding the development and intensity of CF as experienced by EMS practitioners.
Conversely, burnout does not necessarily mean that our world views have been damaged or that we have lost the ability to feel compassion for others. Most importantly, burnout can be easily resolved; (but can it be in the current financially driven, dehumanised environment practitioners work in?)Conversely this is not the case for CF and VT.
As one is vicariously exposed to trauma, both directly and indirectly, one begins to exceed one’s resilience (or ability to cope) to these events, and one is then prone to develop CF (or sometimes also referred to as Secondary Distress Syndrome). Once our chronic exposure to trauma exceeds our coping mechanisms, CF then becomes evident. CF has been described as the convergence of secondary traumatic stress (STS) and cumulative burnout (BO); a state of physical and mental exhaustion caused by a depleted ability to cope with one’s everyday environment. This can impact standards of patient care, relationships with colleagues, or lead to more serious mental health conditions such as post-traumatic stress disorder (PTSD), anxiety or depression.
How do we then best protect vulnerable workers, to prevent not only CF, but also the health and economic consequences related to the ensuing, and more disabling, physical and mental health outcomes. To fully understand CF, we possibly need to move away from theoretical explanations and models and focus on a more relational understanding of professionals lived experience of their own and others’ (patients, peers and family) distress. This would involve a narrower focus on problem solving, via person centred compassionate care. Remember authentic and sustainable self-care begins with you. Understand that the pain and stress you feel are normal displays, resulting from the care giving work you perform on a regular basis.
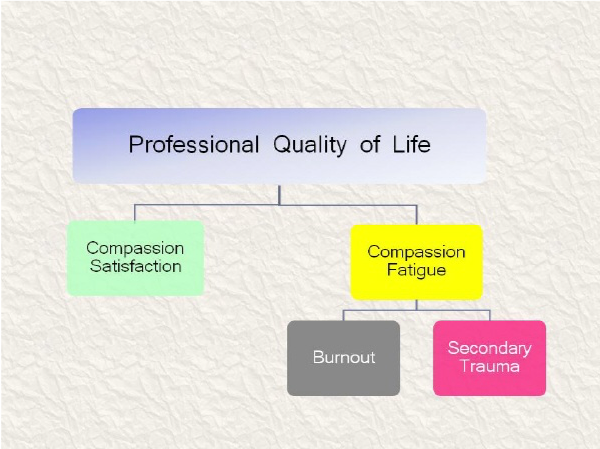
Examine the positive and negative aspects of one’s work influences, and how it affects one’s professional quality of life. This leads us to a better understanding, whilst helping those who experience trauma and suffering. This can in turn improve our ability to aid them and keep our balance in this process.
Compassion Satisfaction and Compassion Fatigue are two aspects of Professional Quality of Life. They encompass the positive (Compassion Satisfaction) and the negative (Compassion Fatigue) parts of helping others who have experienced suffering. Compassion fatigue breaks into two parts. If working with others’ suffering changes you so deeply in negative ways that your understanding of yourself changes, this is vicarious traumatization. Learning from and understanding vicarious traumatization can lead one to vicarious transformation.
Dr. Beth Hudnall Stamm – ProQOL
sessional Quality of Life Model (Stamm, 2012)
An excellent article to read is Transforming Compassion Fatigue into Compassion Satisfaction: Top 12 Self-Care Tips for Helpers, by Françoise Mathieu, M.Ed., CCC– see the link below
In closing;
“integrated intervention programmes are needed to assist EMS personnel working in this sustained high-stress environment. The findings can assist health care educators in the design of co-curricular activities intended to help in the development of resilience and the psychological wellbeing of EMS personnel.”
Exposure to daily trauma: The experiences and coping mechanism of Emergency - Llizane Minnie a,* Q3 , Suki Goodman b, Lee Wallis
Healing begins from within, and being committed to a self-care plan, with clear boundaries in both your personal and professional life and understanding one’s negative behaviours and their root cause. Internal self-healing in our profession is a life-long management plan, but as you continue to do the necessary internal work, life will and can, begin to change for the better.
References, websites and additional reading:
Cocker, F., & Joss, N. (2016). Compassion fatigue among healthcare, emergency and community service workers: A systematic review. International Journal of Environmental Research and Public Health
Hernandez-Wolfe, P., Killian, K., Engstrom, D., & Gangsei, D. (2015). Vicarious resilience, vicarious trauma, and awareness of equity in trauma work. Journal of Humanistic Psychology
Ray, S. L., Wong, C., White, D., & Heaslip, K. (2013). Compassion satisfaction, compassion fatigue, work life conditions, and burnout among frontline mental health care professionals. Traumatology
Sprang, G., Clark, J. J., & Whitt-Woosley, A. (2007). Compassion fatigue, compassion satisfaction, and burnout: Factors impacting a professional’s quality of life. Journal of Loss and Trauma
Mathhieu, F (2017) Transforming Compassion Fatigue into Compassion Satisfaction: Top 12 self-care tips for helpers. Workshop for helping professionals
Minnie L et al. Exposure to daily trauma: The experiences and coping mechanism of Emergency Medical Personnel. A cross-sectionalstudy, Afr J Emerg Med (2015), http://dx.doi.org/10.1016/j.afjem.2014.10.010
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-08 12:34:212019-08-13 11:18:45Compassion Fatigue vs Compassion Satisfaction
A new community paramedic service has been set up in Weardale.
The service started this month and covers Crook, Willington and Stanhope. It will initially operate for a 12-month trial period. The new service is in addition to a similar scheme which currently operates in Barnard Castle.
Paramedics from the North East Ambulance Service (NEAS) are working with local GPs, district nurses and falls teams to provide improved, community-based health care and reduce the time it takes to respond to life-threatening emergencies.
The scheme is a joint venture involving NEAS, NHS Durham Dales, Easington and Sedgefield Clinical Commissioning Group (DDES CCG) and the local GP Federation of doctors.
The paramedic team will use a rapid response vehicle and be available from 8am-8pm seven days a week. They will be work solely in the Crook/Willington/Stanhope area and will respond to immediate life-threatening incidents if they are closest to the patient.
They will also help support GPs by carrying out some home visits and work with other healthcare staff to prepare and deliver care plans for patients with long-term conditions.
Phil Blance, the Clinical Operations Manager for NEAS in the Dales said:
“This new scheme will mean that our paramedics will be much closer to local communities and be able to respond more quickly to the most serious incidents.
“The scheme in Barnard Castle has shown that the number of patients taken to hospital can be significantly reduced – that’s good for patients and helps reduce the impact on the rest of the NHS.”
Stewart Findlay, chief officer of NHS DDES CCG, said: “We have been working hard to find a solution to the difficulties in providing an emergency response to our rural areas for some years now.
“For many years we have invested significant additional money in to the two Durham Dales and the service that now runs in Teesdale offers a solution that is popular with patients and GPs alike.
“It offers the best chance of a rapid response and makes best use of paramedic time which is dedicated to the Dale. It demonstrates how well the CCG has been working with NEAS, our local GPs and our local GP federation and I am delighted to see it now extended to the Weardale population.”
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-08 12:01:142019-08-13 11:19:09Weardale community paramedic scheme starts
Celebrating those who have demonstrated the highest levels of patient care and innovation across Cheshire and Merseyside, North West Ambulance Service (NWAS) has held its second ever Achieving Clinical Excellence (ACE) Awards last week.
The ceremony, which took place on Tuesday 30 July at Formby Hall Golf Club, was hosted by Dave Kitchin, Head of Service. Chief Executive, Daren Mochrie and Chair, Peter White presented eleven awards to individuals, teams of staff and also external agencies. Winners were rewarded for their clinical excellence and achievements over the past year.
Daren Mochrie, Chief Executive says: “The awards are an opportunity to reward our professional employees who are committed to delivering the highest quality of patient care as well as members of the public who have stepped in to make a real difference. As chief executive I am extremely proud to recognise such outstanding achievements.”
The categories and award winners were:
• Consultant Paramedic Award – Leona Blayney, Craig Butterworth, Gary Fitzpatrick, Gareth Owen, Jade Parry, Danielle Shaw
• Advanced Paramedic Award – Wayne Evans, Dylan Hughes, Jessica Heath
• Clinical Leadership Award – Andy Baines
• Supporting Clinical Excellence Award – Cheshire & Mersey Fleet Team
• Mentor of the Year – Paul Campbell
• Student of the Year – Samuel Hebden
• Communication Centre Award – EOC Orange Team
• Innovation and Change Award – Darren Earley
• Patient Choice Award – Sarah Camplin, Andrew Hazley, Michael Jackson, Diane McGann, Aaron Murray, Michael Quirk, Stephen Rickards
• Everyday Hero Award – Total Fitness, Crewe
• The John Harrison Award for Outstanding Achievement – Peter Fisher, Danielle Phelan and Andrew Carter-Sweeney
Winners were selected from peer nominations by a judging panel consisting of Head of Service, Dave Kitchin, Consultant Paramedics for Cheshire and Mersey, Nick Sutcliffe and John Collins alongside the trust’s Medical Director, Dr Chris Grant.
Maxine Power, Director of Quality, Innovation and Improvement chose the winner of the Innovation and Change Award. This was presented to Senior Paramedic Team Leader, Darren Earley who has developed a tool to support NWAS clinicians when treating patients with mental health concerns.
The John Harrison Award is in memory of Dr John Harrison, the trust’s former associate medical director who exemplified the highest clinical standards of care. The recipient of this award was emergency services team, Peter Fisher, Danielle Phelan and Andrew Carter-Sweeney who were recognised for outstanding professionalism when faced with a colleague having a medical emergency. Their award was presented by John Harrison’s wife, Margaret, along with their colleague who thanked the team for their life-saving actions.
Staff from Total Fitness in Crewe were given this year’s Everyday Hero Award. Thanks to their training, quick thinking and use of the defibrillator on site, the team were able to help save the lives of two people in separate incidents just three months apart.
All winners were presented with a certificate and award to recognise their actions.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-08 11:45:522019-08-13 11:19:19AMBULANCE SERVICE CELEBRATES CLINICAL EXCELLENCE ACROSS CHESHIRE AND MERSEY
Three brothers from Newcastle have been awarded bravery certificates by the North East Ambulance Service for their actions in helping to get emergency help for their mum after she collapsed at home.
Seven year old twins Charlie Duke and Dylan Duke, and their four year old brother Jayden Douglas, were at home when their mum Lisa Hefferin collapsed at the bottom of the stairs and became unresponsive.
Dylan rang 999 by using his mum’s mobile but it was Charlie that spoke with call handler Vikki Wightman, to ensure the door was unlocked for the ambulance crew to arrive and that he and his brothers stayed safe.
Vikki said, “The call came in and I was alarmed that it was a young boy ringing about his parent. All three of the boys spoke on the phone and gave a clear account as to what had happened, but it was Charlie that gave me clear details of his mum’s condition and what their address was.
“If children know the basic information of what to do during an emergency, it makes it that little bit easier for us to find out exactly what is going on.
“It was a privilege to be able to award Charlie and his brothers for their actions. They were all so brave in getting their mum the help she needed. It’s not every day we get to see the outcome of a patient and as a call handler, being able to meet the person on the other end of the phone, really puts into perspective the work that we do.”
Lisa suffers with low blood pressure and has to take iron tablets. Her blood pressure dropped so low that day that she collapsed and didn’t regain full consciousness until she was in the back of the ambulance, on her way to hospital.
Lisa said, “It was me and the three boys in the house at the time and it was absolutely amazing what they did. Charlie looked after his siblings and called for help for me when I needed it the most. I couldn’t believe it.
“I think every parent should learn from my story and educate their children in what to do during an emergency. I taught them what to do and they got me the help I needed.
“I’m so proud of all of my sons.”
The ambulance crew members that attended to Lisa were paramedics Craig Hurst, Victoria Landale and Daniel Price as well as rapid response paramedic Paul Jackson.
Craig has worked at NEAS for seven years and has been a qualified paramedic for two and a half years. He remembers the job well, “We got a serious life threatening call about a female in cardiac arrest at her home and that one of her children had called 999.
“When we arrived he had unlocked the door for us and we saw Lisa in a semi-conscious state. Thankfully she wasn’t in cardiac arrest. Charlie had found blankets and pillows to make his mother comfortable and stayed by her side the whole time. Whilst we were there he was looking after his brothers and gave us exceptional information about what had happened. As it turned out, she collapsed with low blood pressure.
“He continued to look after his brothers and got them ready for school whilst we were helping Lisa and kept their family dog calm.
“I feel the efforts of this young gentleman and his brothers deserve recognition and I could not go without presenting them a bravery certificate.”
Victoria Landale has worked at NEAS for five years, first beginning as a dispatch officer in in the emergency operations centre. She said, “It’s great to meet Lisa and to see how she is getting on from what happened. It’s also closure for us to hear the outcome of patients that we have treated, which we don’t always get to hear about.
“Many schools now are implementing CPR within their curriculum and I think this case highlights the simple things that young children can do to save their parents or someone else’s life.”
Daniel Price said, “Charlie was a really grounded little boy as he kept reassuring his brothers that mummy was going to be alright. He also got them ready for school, he was really mature for his age.
“We don’t get a thank you very often but when we do it’s really nice to get one. My job is to help people and when someone recognises that, it’s really inspiring for me.”
The Trust is hosting a CPR training day called Restart a Heart Day in October, that encourages schools, organisations and communities to sign up to receive lifesaving skills in CPR.
Over 30,000 people suffer a cardiac arrest out of hospital in the UK every year. Currently, less than one in 10 survive. The earlier a patient can receive CPR and a shock from a defibrillator, the greater their chance of survival. We know that the major difference is widespread training in CPR. Find out more and sign up to Restart a Heart Day: http://bit.ly/2L7UJFF
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-07 14:11:192019-08-13 11:19:32Brothers rewarded for their brave efforts in getting their mum emergency help
Published in Spring 2019 Edition of Ambulance Today Magazine
In this column, Jerry Overton- who is viewed by many world EMS and healthcare leaders as one of the best when it comes to improving ambulance systems globally- gives his opinion on the allocation of funding in theEMS system. He identifies some of the issues within EMS systems globally and, whether it’s saving ambulance hours or reallocating funds, you can trust Jerry to have a pretty good idea on how to improve on the system.
Oh, a storm is threat’ning
My very life today
If I don’t get some shelter
Oh yeah, I’m gonna fade away
-“Gimme Shelter”
Yes, it is a storm that is constantly threatening, and it threatens us all. Cardiac events know no shelter; they do not “fade away”. How sadly ironic it is that the emphasis on this issue of Ambulance Today is the recent London Cardiac Arrest Symposium last December, an event that Dec, lover of the Rolling Stones, had planned to cover. This all still just does not make any sense.
As always, the symposium was excellent, and I am sure the specifics will be comprehensively reported elsewhere. From this perspective, the welcome change was less on research and more on resources; human resources. The first, “Community CPR”, and second, “Kids Saving Lives”, really hit the mark.
This does not mean that cardiac research is not important, because itis. But, at the end of the day, whenone considers the amount of money committed to research compared to the amount of money needed to increaseour resources, one wonders if it is not time to discuss priorities.
Back in the day (okay, my day), the initial intervention for an out of hospital cardiac arrest was the precordial thump and if that did not work, there was always intracardiac epinephrine and sodium bicarb. Other meds came and went, depending on the latest research, and sometimes even who did the research. The contents of the drug box varied from system to system and the decisions of the local medical director. Sadly, ROSC rates failed to show any real improvement, whether in the United States, the United Kingdom, or Asia.
Today, every responder knows that two interventions make a difference, timely CPR and timely defibrillation, stressing the word “timely”. The question now, though, is what constitutes “timely”. It sure is not an eight-minute requirement. As has long been stressed by any paramedic, there will be little difference in outcome if the response time is 9 minutes 1 second rather than 8 minutes 59 seconds.
Response times are outputs, and what is needed are outcomes. And to achieve outcomes, we need resources. That, clearly, requires our most important resource, which is our people. If we really do have money for new programs, it is time to invest in the “research” necessary to seriously examine howwe can better recruit and retain those that can change patient outcomes. And if we do not have any “new”, perhaps reallocation of funds is in order.
There can be no debate that shaving seconds in telephone CPR instruction is important, but if there are insufficient dispatchers to answer the increasing number of calls, those seconds will make little difference. It is an under appreciated, almost invisible position, that drives the first link of the Chain of Survival.
The shortage of paramedics is even more acute. In the U.K., a 2017 report by the Comptroller and Auditor General of NHS England, reported 10 percent vacancy rate, with Trusts “struggling to recruit the staff they need and then retain them.” The U.S. is facing a similar problem. A recent broadcast from CNBC news reported that in the next six years, a 15 percent increase of paramedics would be required at a time “when unemployment continues to hover near historic lows”.
Of course, it is not just the out of hospital care world that is facing a crisis, other sectors of health care are also, and it directly impacts our ability to respond. That same 2017 report by the Comptroller and Auditor General found that in “2015-16, approximately 500,000 ambulance hours were lostdue to turnaround at accident and emergency departments taking more than 30 minutes, which equates to 41,000 12-hour ambulance shifts.”That is an almost unbelievable (but it is) staggering waste of both human AND financial resources.
Longer hours, more responsibility, higher utilization, fatigue, inequitable pay, and, of course, working conditions when considered together would make any sane person wonder why another sane person would ever consider makingthe commitment to a dispatcher or paramedic. The answer is, obviously, EMS personnel give a damn.
All too often, that is forgotten. It was just under three years ago that the first European congress dedicated to EMS was held in Copenhagen, EMS2016. The theme of that congress, and the subsequent congresses, was “It takesa system to save a life,” and indeed,it does. But the foundation for that system, or any system, is its people. In other words, without you, it is nothing.
That is my point. If we are ever to increase cardiac arrest outcomes,it will be done by human resources that have the education, experience, and motivation to make a difference. Telephone CPR does little good if a call goes unanswered. A medication has little impact if there is no paramedic to administer it.
Just like human resources, economic resources are limited. And it is a basic tenet of EMS that “nothing in life is free”. That includes community and kids’ CPR. Wisely using the financial resources that we do have is key, and if that means reallocating research grant funds away from the latest in drone delivery systems that could potentially increase survival one-half of one-half percent (yes, that is sarcasm), it needs to happen if those same funds can help us better find the keys to retain the human resources that WILL make a difference (No, I am not naive, higher wages is definitely a major key!!!).
And just when you think that all of us have at least a basic understanding for the need for a resource, any resource, that can respond and make a difference, comes this from the western section of the United States. It seems that officials in a Pacific Northwestern state have decided that call taking in dispatch centers has become so structured, and telephone CPR so protocol driven that they are proposing a rule change that would permit local agencies to no longer require its dispatchers to be certified in CPR. Yes, you read that correctly, public safety responders will not need to know CPR.
It is not like a fellow dispatcher has not arrested in a control center, because it has happened. It is notlike a fellow public safety officer has not arrested at headquarters, becauseit has happened. And it is not likea dispatcher has never witnessed a cardiac arrest as a layperson, because it has happened. Whether the proposal passes will be decided in early spring. And, interestingly, most local public safety agencies are AGAINST it. Perhaps those state officials need to take a step back and consider this from the Rolling Stones. It certainly fits.
You can’t always get what you want
You can’t always get what you want
You can’t always get what you want
But if you try sometimes well you just might find
You get what you need
“You Can’t Always Get What You Want”
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-07 13:05:312019-08-13 11:19:54"Waiting on a Friend"
Published in: Summer 2018 Edition of Ambulance Today Magazine
Magen David Adom (MDA), Israel’s National EMS organisation and Blood Services provider, is also Israel’s largest volunteer organisation. On its way to gaining this formidable title, MDA has taken upon itself the vital role of educating not only its employees in basic and advanced life-saving skills, but also a large number of Israel’s general population. Youth, medical staff and many others from around the world benefit from Magen David Adom’s professional and experienced trainers.
Our youngest volunteers are 15-years-old, and begin studying towards a First Aid Provider certificate that allows them to volunteer on front-line ambulances. Often these teenagers undertake this course as part of a national volunteering scheme which requires all of those leaving school to have served a certain number of volunteer hours in order to receive their matriculation certificates.
MDA volunteers go well beyond their required hours, with just the 60-hour course itself almost entirely filling their quota. Nevertheless, many of the young volunteers work several times a week in eight-hour shifts, assisting the EMS crews in their life-saving duties.
These young volunteers often run training sessions of their own, either for the next youth volunteers or for members of the public, at CPR stands in malls, train stations, schools and other public places.
Within the MDA framework, there are other short courses provided to the general public, beginning with a 22-hour “Life Guardian” course. This teaches the basic life-saving skills required in order to begin treatment in life-threatening cases such as cardiac arrest. Volunteers on this scheme are provided with basic life-saving equipment and then download an “MDA Teams” mobile phone app that notifies them if there is a call nearby and sends them details of the address and nature of the incident. This has helped to reduce response times in many cases to a matter of seconds, thus increasing patients’ chances of survival.
Courses provided to medical staff are conducted around the country, both in their medical facilities and in MDA stations. These courses include refresher courses, Basic Life Support (BLS) courses, Advanced Cardiac Life Support (ACLS) courses, and tailor-made training sessions.
ACLS, PHTLS and PALS courses are all run under the auspices of the American Heart Association, with MDA being one of the few non-American organisations with AHA accreditation for running their courses and issuing certificates. These courses are run across the country for nurses and doctors who are required to attend refresher courses every two-to-three years.
Magen David Adom runs several courses a year aimed at international teams of doctors who come to Israel to learn from the wealth of MDA’s experience particularly, but not exclusively, in the field of mass casualty incidents. There have been teams from as far apart as France, Canada and Mexico who have joined specialised courses set in an Israeli background. There are, of course, EMT courses being constantly run, providing a flowing stream of qualified staff, including both volunteers and employees, for our ambulances.
Arguably, the pinnacle of Magen David Adom’s education services lie within the Paramedic Education Centre, located in MDA’s Ramat Gan station, but branches are located all across the country. All of Israel’s Paramedics undertake their training with Magen David Adom, either in part or in its entirety, regardless of which course or courses they may have joined. There are courses for volunteers, EMTs who wish to take the next step in their career, military Paramedics, university degree Paramedics, those who are undertaking their national service in MDA, and many others. There have been courses run for all sections of society, irrespective of gender, race or religion, often tailored towards specific communities.
These communities, such as the Bedouin and Ultra-Orthodox communities, are underrepresented in the ranks of EMS in general, including Paramedics in particular. Providing each community with dedicated conditions allows their members to study in ideal conditions to complete the prestigious Paramedic course, and begin serving not only their communities, but the general public as a whole.
Magen David Adom strives to educate as many people as possible in our primary, life-saving mission. We welcome all those who wish to learn to join us and be part of our education agenda. As it says in our logo – It’s a Matter of Life.
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-07 11:53:492019-08-13 11:20:11MDA Education: The skills to save a life
Published in: Summer 2018 Edition of Ambulance Today Magazine
At the end of 2014, and early 2015, we went through a period of industrial action in the NHS over pay involving two 4-hour stoppages. In the ambulance sector, many staff were not prepared to come to work, even under emergency life and limb cover arrangements. This led the government to put the army on standby. So, what happened and what have we learnt?
Why were staff not prepared to come in? Well the answer lies in the fact that ambulance staff have been raising issues with workload, pressure, demand and lack of support for a number of years. Trouble was no one was listening. Performance dominated Trust boards and finance fixated commissioners missed the warning signs.
Here came an opportunity for staff to make themselves heard. They voted with their feet in the knowledge that their legal right to take lawful industrial action would protect them. When it came to settling the dispute, we made sure that ambulance staff wellbeing was part of the final settlement.
So, what has happened since then? Well, we have been working to develop a collaborative approach between Ambulance Employers, Trade Unions and NHS Employers to improve the mental health and wellbeing of the ambulance services workforce.
We started by bringing together staff and employers to discuss the challenges each group faced. We have to recognise, whether we agree or not, that there is a policy of austerity in government meaning budgets are increasingly tight and the expectation is that employers will do more with less. However, this policy leads to problems for employers as staff leave jobs for less stressful and better paid work leading to recruitment and retention problems.
Employers listened to staff concerns about working conditions, not just for the operational staff working on ambulances, but also the staff working in the contact centres and corporate services. Fewer people doing more work in an increasingly challenging environment. This is not easy listening for employers, many of whom work in managerial roles to help support staff in the delivery of 999, 111 and PTS services. Ultimately, they have little control of the government’s public sector funding policy.
However, they do have to deal with the consequences – the dropping job satisfaction, morale and motivation; the loss of organisational commitment and discretionary behaviour. This leads to a worsening engagement, stress symptoms and burnout. Then they have to account for increasing absence rates and unfilled shifts.
At first it seems like an impossible puzzle with too many pieces that don’t seem to fit together. How do you improve wellbeing, especially when you know what is making people unwell, but it feels out of your control and when taken as a whole it seems an impossible task?
We started by grouping the pieces of the puzzle together based on the key issues.
Mental health and resilience. Helped by Mind and the Blue Light Programme we know that ambulance staff are more likely to suffer from mental health problems but less likely to do anything about it.
Bullying and harassment. Whether it is a manager and staff relationship, a control and road relationship or a hospital and ambulance relationship, we know they are already strained. Cultures in ambulance services need to change. External and internal pressures lead to poor behaviour but we need to eliminate bullying.
Reducing violence and aggression. Too many times we read reports about staff being assaulted. I have written about this subject before and no one disagrees - we need to tackle this issue. With the right focus on prevention and prosecution we can reduce the harm caused by violence.
Leadership behaviour. Ambulance staff take on managerial roles and then are not given the support or training needed to discharge their duties. We hear of senior management teams that are out of touch with staff. Line managers have a major role in supporting and developing staff. Senior management need to give them the training, autonomy and trust to support their staff.
Working patterns and role design. Ambulance work takes years off your life! More and more evidence shows us that long hours, shift working and night working is bad for us and leads to preventable diseases. Some staff like working longer shifts to get longer periods of time off, but with no guaranteed meal breaks and the likelihood of a long shift overrun it’s time we looked seriously at this issue to make work less demanding but recognising peoples’ needs to spend time with their friends and family.
Equality and inclusion. The experience of BME ambulance staff is of inequality in career progression, increased experiences of harassment and bullying and underrepresentation at senior level.
Recognition and staff engagement. Each year the NHS Staff Survey shows how poorly engaged ambulance staff are. They are the lowest scores across the NHS. I do not honestly think it is deliberate but you get very little recognition for a job well done, whereas you do hear about a missed performance target or a complaint. Ambulance services need to get better and reap the rewards of telling staff they recognise the effort they are making, especially in difficult times.
Healthy lifestyles. Last but by no means least. Ambulance work does not lend itself to healthy lifestyles. Shift work, late night snacking on poor quality food, combined with lack of consistent exercise and the physical demands of the job are a bad mix. However, looking after your own health is important and we want to see more employers supporting staff to live more healthily.
The real trick for the national bodies, employers and trade unions will be getting the buy-in from staff and for them to trust that this is more than just a new initiative. The benefits are proven and what we have been saying for a long time. To get good patient care you need to start with good employee care. At the end of the day, healthier happier staff = healthier happier patients.
Published in: Spring 2019 Edition of Ambulance Today Magazine
EMS staff have enough to deal with when responding to a call, the last thing they need is members of the public making harder work of it. In this column, Thijs Gras explains the difference between ‘innocent inquisitiveness’ and ‘sick sensationalism’ when it comes to the scene of an accident.
We got a call: probable resuscitationin a tram. When we arrived we founda man of about 70 years lying on the ground in a tiny space inside the tram. It was cold and rainy, so carrying him outside was not an option, at least not without proper preparation for which we had no time. The police were already performing CPR, all the passengers were out of the tram. We pulled the man a little under to create a bit more space and took over the resuscitation. While I was ballooning the man I suddenly noticed someone on the outside, looking curiously through the window of the tram as to what we were doing there.I was amazed and so were the police. After this guy was chased away, only a couple of moments later a woman took over. She gazed inside.
Now I must admit I have a certain degree of understanding, people being inquisitive when something happens involving lights and sirens. Mankind is naturally curious. In my younger years hearing the fire service acceleratedmy heartbeat and if I knew where they were going to, I went as well. A fire is fascinating to see. Smoke and flames, lights and sirens attract attention, which generally is okay, as long as you do not come too near or hamper rescue and/or fire fighting operations.
Labelling it positively, one could referto this as interest in the community, in society, in other people. The attraction could even have an evolutionary use: it is a way to mobilize help and assistance. It is only relatively recently that rescue and emergency medical care outside the hospital is professionalized and trusted to specially trained people from dedicated organizations and services. But even nowadays we value first responders and bystanders because they have one big advantage over the professionals: time. Professionals need to be informed there is a problem,find out where it is and who shouldbe handling this, and then alert the required units to rush to the scene. All these steps take time, so having people around to extinguish a fire, control a bleeding or perform CPR may be of great value.
But there are boundaries. Some people prefer filming to rendering first aid.This is ridiculous of course. Even after emergency services arrived on the scene and are doing their job, people may come very close, sometimes too close for comfort. Being a historian, I went through a lot of pictures of accidents. One would be amazed by the number of people watching accidents on some of the older pictures. Apparently this is of all ages. In the Netherlands we call this ‘disaster tourism’.
But do not forget, it may be dangerous! Even in The Netherlands we had a nasty experience in this field with the big explosion of a firework factory in the town of Enschede in May 2000. Among the 22 fatalities (including four fire fighters) and about 950 injured, were a number of people that had come to the incident just out of curiosity.
In recent years cell phones and iPhones have taken sensationalism a step further; everything is filmed nowadays. You make your own reality TV and broadcast it among your friends or nasty news channels. With a bit of luck your footage goes viral.
Last year in August there was a big collision on one of the Dutch highways. One person was so seriously injured he had to be resuscitated. People were filming everything. They bashed through the accident scene trying to get the best pictures, destroying important marks for the police investigation. They used lanes, marked with red crosses. A car even stopped on the opposite side of the motorway to film the accident, almost causing another accident with an oncoming lorry. Police noted as many registration plates as possible to give these people a big fine. Will they learn?
There are thin lines between innocent inquisitiveness, caring curiosity,sick sensationalism and pathologic papparazionism. The first two are relatively okay and can be dealt with, the other two are not okay and refutable.
As ambulance crews we
ask the right honourable members of the public not to film patients and victims.
And if you are struggling against the temptation, just reflect before you film:
“What if this was me or my mother or my father? Do I want to go viral?”
Accidents are no film sets. . .
https://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpg00Joe Heneghanhttps://ambulancetoday.co.uk/wp-content/uploads/2019/09/AT-Logo-2-1-300x68.jpgJoe Heneghan2019-08-06 18:48:372019-08-13 11:21:04Accidents are no film set
We may request cookies to be set on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience, and to customize your relationship with our website.
Click on the different category headings to find out more. You can also change some of your preferences. Note that blocking some types of cookies may impact your experience on our websites and the services we are able to offer.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to deliver the website, you cannot refuse them without impacting how our site functions. You can block or delete them by changing your browser settings and force blocking all cookies on this website.
Google Analytics Cookies
These cookies collect information that is used either in aggregate form to help us understand how our website is being used or how effective our marketing campaigns are, or to help us customize our website and application for you in order to enhance your experience.
If you do not want that we track your visist to our site you can disable tracking in your browser here:
Other external services
We also use different external services like Google Webfonts, Google Maps and external Video providers. Since these providers may collect personal data like your IP address we allow you to block them here. Please be aware that this might heavily reduce the functionality and appearance of our site. Changes will take effect once you reload the page.